
Why to Choose the Volume Clamp Method for cNIBP over Other Methods
Date: 19th January 2022
Reading time: 8 - 10 mins
Author: Gerard Langewouters, founder of Finapres Medical Systems B.V.
In this blog post, different methods for continuous non-invasive blood pressure (cNIBP) measurement are being discussed. The key discussion points are:
- The milestones in continuous arterial blood pressure measurement
- The cuff-based techniques to determine cNIBP: the Volume Clamp technique and Applanation Tonometry
- The cuffless techniques to determine cNIBP: Pulse Transit Time, Pulse Wave Analysis, and Pulse Decomposition Analysis
- Why the volume clamp method prevails over other cNIBP techniques
Key Milestones in Continuous Arterial Blood Pressure Measurement
Arterial blood pressure (BP) is one of the vital parameters most often measured in clinical practice. A remarkable scientist, Carl Friedrich Wilhelm Ludwig (1816-1895), invented the kymograph in 1847, which for the first time enabled the graphical recording of continuous oscillations of human arterial pressure [1].
In 1949, almost a century later, intra-arterial BP monitoring through an arterial line was first used clinically [2], thereby facilitating more in-depth study of human physiology. However, arterial lines are only indicated in seriously ill patients in the intensive care unit or during surgery in the Operation Room.
In the past 50 years, continuous non-invasive techniques have been developed to provide alternatives to invasive blood pressure measurements. Such techniques can basically be divided into:
- cuff-based techniques and
- cuffless measurement methods.
Both methods are briefly described in this blog post, together with their pro’s and con’s.
1.Cuff-based Techniques to Determine cNIBP
Two major cuff-based non-invasive techniques are:
- Applanation tonometry and
- Volume-clamp technology
Applanation Tonometry Technique for cNIBP
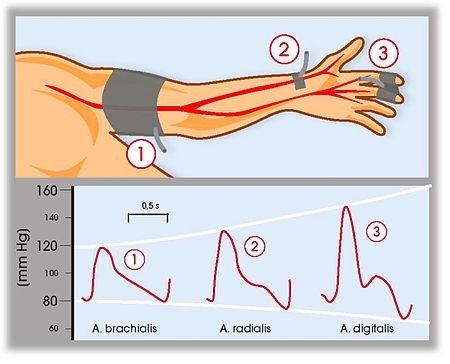
In 1963, Pressman and Newgard developed arterial tonometry [3]. Tonometry measures arterial pressure by applying force over a superficial artery (e.g. the radial artery) to distort the vessel. This can be performed through a wristband or with a hand-held instrument and records pulsatility from applied force flattening the chosen superficial artery.
The manometer-tipped probe must flatten or applanate the artery against a bone so that its wall tension is perpendicular to the probe. At this applanation state, the tangential arterial wall tension does not affect the vertical force measured using the transducer. Therefore, after some simplification and assumptions, the measured arterial displacement due to arterial pulsation are regarded to be proportional to the intra-arterial pressure. Subsequently, the arterial waveform and continuous noninvasive BP can be derived.
Applanation Tonometry Technique Challenges
Manual and automatic applanation have proven to be difficult. Practical problems such as sensor positioning, motion artifacts, and calibration are encountered. Tonometry methods can become problematic as they are sensitive to imprecise placements of the device and easily result in inaccurate readings, especially with patient movement. Continuous control of the positioning of the tonometer is needed, while the subjects need to be in a supine position during monitoring [4]. Establishing a calibrated baseline of tonometry BP readings remains challenging. As a result, in practice the measured waveform has to be calibrated with cuff BP whenever a blood pressure change is anticipated.
Although radial artery Applanation Tonometry has a sound physiologic basis and hence potential in the arena of clinical medicine, published treatment and outcome data for it are less complete than for brachial blood pressure [5]. On the other hand, arterial tonometry has been improved to be reliable and commonly used in the measurement of pulse wave velocity (PWV) for the evaluation of arterial stiffness.
Volume Clamp Technique for cNIBP
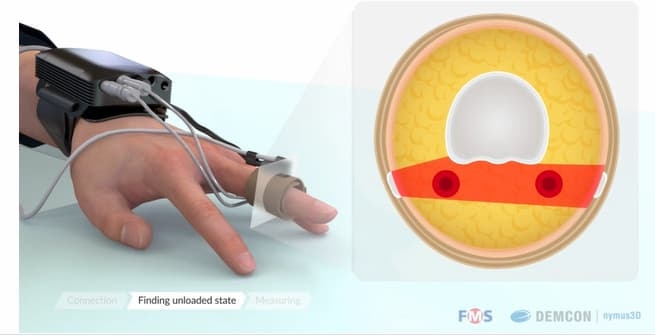
In 1973, approximately 10 years after the development of arterial tonometry, Jan Peñáz, a Czech physiologist, developed the volume clamp method for unloading the finger arteries by applying external pressure to the finger using a cuff with an inflatable bladder, in order to measure the continuous blood pressure in the human finger non-invasively [6].
The system includes an inflatable finger cuff with a built-in photo-plethysmograph (PPG) sensor, a fast pneumatic servo system, and a dynamic servo setpoint adjuster. By using the fast servo system, a pulsating cuff pressure is applied to the finger arteries that are precisely opposite to the intra-arterial pressure. Through the process of unloading the arterial diameter to a setpoint, the artery is clamped at a constant size reduced from its elastically expanded and pulsating diameter to a smaller non-pulsatile diameter.
When the cuff pressure equals the arterial pressure, the transmural pressure, which is the difference between the intra-arterial pressure and external applied cuff pressure, is zero. Unloading of the artery until its diameter equals the unstressed diameter is crucial for the volume clamp method of Peñáz. To ensure this, the criterion for the correct setpoint should be based on the physiological properties of finger arteries. The automated physiological calibration (Physiocal) invented by Karel Wesseling made it possible to keep track of the correct setpoint level of the continuous non-invasive finger blood pressure, even during changes in vascular tone of the finger arteries [7].
The first commercially available volume-clamp based Finapres device was introduced in 1986. Since then, a range of devices based on the volume clamp technology has become available from different medical device companies. Finapres Medical Systems has introduced several devices, such as Portapres®, Finometer® and the currently available Finapres® NOVA devices with the NANO CORE® technology (read more about this in the blog Finapres®, an Innovative History).
These devices are equipped with a so-called height correction system to automatically correct the finger blood pressure for hydrostatic blood pressure changes induced when the measured hand is moved away from heart level. Moreover, these devices do not only provide non-invasive finger blood pressure, but also reconstructed brachial artery pressure using an inverse filter technique. In addition, arterial pressure waveforms indicate changes in the cardiovascular status, allowing the approximation of additional derived parameters such as stroke volume, cardiac output, arterial stiffness, and vascular resistance on a beat-to-beat basis.The availability of continuous non-invasive blood pressure measurement has contributed, among others, to broaden the body of physiology-based knowledg in the area of syncope, short-term blood pressure control, and cardiovascular reflex activity (read more about this in the blog “Get to know the Syncopedia Foundation: the Syncope Knowledge Facilitator!”).

2.Cuffless Techniques to Determine cNIBP
In the last two decades, significant investigations have been performed on continuous or beat-to-beat BP measurements without any interruption for unobtrusive application without the use of a cuff. The BP is estimated by processing signal features, so-called surrogates, which are modulated by variations of BP. These techniques include well-known approaches such as pulse transit time (PTT), pulse wave analysis (PWA), pulse decomposition analysis (PDA) or combinations thereof.
Pulse Transit Time Technique for cNIBP
Pulse transit time (PTT) is the time taken for the arterial pulse pressure wave to travel from the aortic valve to a peripheral site. More general, PTT is defined as the time taken by a pulse wave to travel between two places in the cardiovascular system.
The pressure dependency of arterial properties is at the base of the cuffless technique employing pulse transit measurement as an attractive surrogate measure of cNIBP.
The PTT-based approach for cuff-less BP monitoring involves the following three steps:
- measurement of proximal and distal arterial waveforms;
- estimation of PTT from the waveforms; and
- calibration of PTT (in units of ms) to BP (in units of mmHg).
Pulse Transit Time Technique Challenges
There are several challenges in successfully implementing these steps. The greatest challenge is calibration. Although it is proven that PTT has a strong correlation with the systolic and diastolic blood pressures, this relation is highly dependent to each individuals physiological properties. The calibration curve relating PTT to BP is dependent on the distance between the waveform measurement sites, blood density, the average cross-sectional area of the arteries between the measurement sites, and the precise function relating BP to arterial compliance. Except for blood density, these parameters are all subject-specific. A calibration curve that is tailored to each subject would be optimal. However, constructing such a curve requires cuff-based BP measurements from the subject.
Another major challenge of PTT is convenient waveform measurement. PTT can be determined using different sensing approaches such as electrical, optical, mechanical, bioimpedance, and magnetic sensors. For convenience, a combination between ECG and (finger-)PPG signals is the most commonly-used pair to derive PTT value. The starting point of the time delay is the R-peak of ECG, while the ending point varies from the peak of PPG to the first/second derivative of the PPG signal.
Determination of BP using the PTT is strongly influenced by the quality of the electrocardiogram and finger plethysmography. There are several reasons for disturbance of electrocardiography signals, which lead to missing or false detection of the R wave, such as electrical noise, movement artifacts, small R wave, and pathological R waves [8]. In addition, the plethysmographic signal can be disturbed, for example by movements, respiratory events, or other events resulting in changes of the hydrostatic pressure.
In summary, therefore, the two biggest practical challenges to measure cNIBP using PTT based technique are the need for frequent calibration as well as the susceptibility to motion artifacts of electrophysiological and PPG signals in daily life. These challenges need to be overcome before PTT-based methods can be applied to routine diagnosis procedures.
Pulse Wave Analysis Technique for cNIBP
Pulse wave analysis, or PWA, is a technique based on the morphological analysis of blood pressure waveforms, whose shape reflects crucial information on the properties of the arterial wall and blood pressure itself [9]. The PWA technique gained interest when applanation tonometry was developed in the 1960s. More recently, PWA has been increasingly applied to photoplethysmographic (PPG) signals, due to the interest in deriving blood pressure-related information from PPG signals routinely measured in clinical settings.
Proprietary PWA algorithms extract features from each pulse based on the wave reflection theory of the arterial system. Such algorithms assume that arterial pulses propagate along the arterial tree being reflected at each arterial branching. The resulting arterial pulses are thus the superposition of forward and backward waves interfering at various locations of the arterial tree. Given the arterial topology of a particular patient, changes in blood pressure modify the velocity at which arterial pulses propagate, reshaping the individual mixture of forward and reflected waves.
These morphological changes are quantified via proprietary PWA algorithms as modifications of the patients’ arterial pulsatility patterns. Pulsatility pattern changes are indirect indicators of the underlying changes in propagation characteristics, and thus, of the underlying changes of central blood pressure. Therefore, the outcome of the PWA algorithm is a number of physiologically meaningful features containing information on the patient’s central blood pressure status.
Novel optical technologies rely on the extraction of physiology-based pulse wave analysis (PWA) features from raw transmission photoplethysmographic signals. These physiological features are later projected into blood pressure values by means of intermittent oscillometric measurements provided by a brachial cuff.
Pulse Decomposition Analysis Technique for cNIBP
Pulse decomposition analysis (PDA) uses a pulse contour analysis approach to quantify hemodynamic parameters such as blood pressure and arterial tone changes. It is based on the concept that two central reflection sites are responsible for the shape of the pressure pulse envelope of the upper body.
The two reflection sites, one located at the aortic juncture of thoracic and abdominal aortas, and the other at the iliac bifurcation, reflect the primary left ventricular ejection pulse to give rise to two reflected and two re-reflected component pulses. Within the pulse pressure envelope of each cardiac cycle these five component pulses arrive sequentially in the arterial periphery. Quantification of the temporal and amplitudinal behavior of the first three component pulses establishes a formalism that can be used to monitor certain hemodynamic states and their changes.
Why The Volume Clamp Method Prevails Over Other cNIBP Techniques
Although significant progress has been made in developing unobtrusive cuffless cNIBP monitoring techniques in the past two decades, most of them are still in their prototype stages. Devices based upon such techniques are usually smaller and lighter than devices using cuff-based technology and measurements are relatively more user-friendly than conventional of cuff-based noninvasive measurements. However, issues such as accuracy, calibration interval, and effect of heart disease remain to be addressed to enhance the reliability and robustness of these techniques for clinical use.
Despite a long research history, the cuffless methods have not yet found widespread use in clinical and ambulatory practice, in part due to technical limitations and the lack of a standardized regulatory framework. Because of the multidisciplinary nature of the cuffless technology, future development will greatly rely on advances in different areas such as novel sensing, physiological modeling, and data analytics.
To date, the vascular unloading concept has been the most successful and validated technique for cNIBP monitoring, bridging the gap between conventional upper arm cuff BP measurements and arterial lines.
For more information do not hesitate to contact us!
References
- Ludwig. (1847, Beiträge zur Kenntnis des Einflusses der Respirationsbewegungen auf den Blutlauf im Aortensysteme (in German, “Contribution to Knowledge of the respiratory movements influence to the aortic system circulation”). 242-302. Available: http://www.biodiversitylibrary.org/item/50159#page/464/mode/thumb
- Peterson, R. Dripps, and G. Risman, “A method for recording the arterial pressure pulse and blood pressure in man,” American Heart Journal, vol. 37, pp. 771-782, 1949.
- Pressman and P. Newgard, “A transducer for the continuous external measurement of arterial blood pressure,” IEEE Transactions on Bio-medical Electronics, vol. 10, pp. 73-81, 1963.
- Solmaz Rastegar, Hamid GholamHosseini, Andrew Lowe. Non‑invasive continuous blood pressure monitoring systems: current and proposed technology issues and challenges. Australasian College of Physical Scientists and Engineers in Medicine 2019. doi.org/10.1007/s13246-019-00813-x.
- Matthew R. Nelson, MD, MS, Jan Stepanek, MD, MPH, Michael Cevette, PhD, Michael Covalciuc, MD, MPH, Todd Hurst, MD, and A. Jamil Tajik, MD. Noninvasive Measurement of Central Vascular Pressures With Arterial Tonometry: Clinical Revival of the Pulse Pressure Waveform? Mayo Clin Proc.2010 May; 85(5): 460–472. doi: 10.4065/mcp.2009.0336
- Peñáz, J. “Photoelectric measurement of blood pressure, volume and flow in the finger”. Digest 10th Conf. Med. Biol. Engng., 1973: 104.
- Wesseling K H, De Wit B, Van der Hoeven G M A, Van Goudoever J, Settels J J. “Physiocal, calibrating finger vascular physiology for Finapres”. Homeostasis 1995;36: 67-82.
- Hennig, A. Patzak. Continuous blood pressure measurement using pulse transit time. Somnologie 2013. DOI 10.1007/s11818-013-0617-x
- Nichols W, O’Rourke M, Vlachopoulos C. McDonald’s blood flow in arteries: theoretical, experimental and clinical principles. CRC Press; 2011, ISBN 9780340985014.